1. Introduce yourself
2. Tell the subject that you want to examine the patient in which no pain will be felt by the patient, and if the patient feels pain then you will stop the examination.
3. Check gross vision by counting fingers at 1 meter.
4. Torch examination
1. Hirshberg test (Tropias)
2. Check pseudostrabismus
3. Abnormal head posture
4. Pupil (Direct and consensual reflex)
5. Epicanthus , telecanthus
6. Nystagmus
7. Ptosis
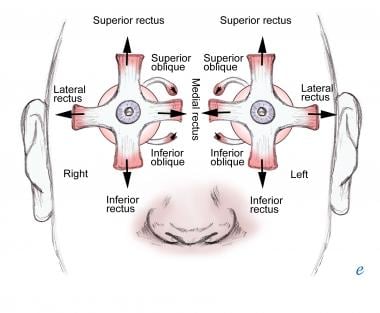
5. Extraocular movements
a) Tell the patient that if he feels any pain or double vision then he/she should speak out.
b) Fixate the eyes of patient on a target like your finger, tip of pen or a torch
c) Move the target in 9 cardinal positions

Tips : Separation of images is greatest in the direction in which the weak muscle has its purest action
d) Hold the target in each position for atleast 5 seconds and observe for any deviation or nystagmus.(Do not take to the extreme positions to make the patient the patient uncomfortable)
e) Perform Saccades by asking patient to rapidly fixate on 1st on one target then on another target like 1st on your finger and then on a pen or torch light.
Tips : Saccadic movement is useful in diagnosing internuclear ophthalmoplegia.
f) Repeat the above step in both horizontal and vertical directions.
g) Test Convergence by moving the target form 1/2 meter away towards the patient and asking the patient if he sees the target double or blurry. (Normally the near point is 10cm after which the patient may see the target blurry or double)
Tips : Do not confuse convergence insufficiency with accommodation insufficiency.
Say Thanks to the patient
Sequence: Observation > Pursuit Movements > Saccades > Convergence
Some Books mention cover/uncover test and krimsky test under ocular motility test however these tests have been covered else where on this website.
Comments
Post a Comment